IT Band Syndrome Anatomy Investigation
#itb #glutes #hamstrings #quads
She saw the finish line! Unfortunately, it was mile 11 of a 13.1 mile half marathon, and the last two miles went inland and then back to the coast. The already exhausted runner contemplated hopping the fence to take a shortcut through the grass. Except – there might be snakes in the tall grass, and there was a Ghirardelli chocolate station at mile 12. So inland it was. The training schedule for her first half marathon was week over week incremental mileage, building up to the day of the Nike half marathon in San Francisco. To maintain basic cardio performance, it is recommended to do some kind of endurance exercise at least 30 minutes a day, for a minimum of 2-3 days a week. If you skip a whole week of training for any reason, you may need to repeat that beginner, cruel, cardio adaptation in the body. So even when there is a minor injury, keep running. The pain will just go away. It didn’t. The body can tweak biomechanics to avoid putting pressure on the area of pain in order to finish the race. But the pain is a warning, and the subtle adjustments to avoid pain can create their own structural issues. By the time you experience IT band syndrome, a myriad of micro adjustments to avoid pain signals have likely taken place in various locations throughout the lower body. This article discusses a detailed investigation of anatomy related to multiple potential components of IT band syndrome. It is likely that the overall function of the lower body is out of sync, and reestablishing core balance will be the long-term solution.
How do people describe IT band syndrome? It hurts- a LOT. So much so that any running is too painful, and the lateral knee burns.Foam rolling and rest are the common suggestions on the internet to alleviate the pain, but that plan is only focused on the dense ITB fibers that travel down the outside of the thigh. This article can end now if I am presenting information already known about the IT band by the general public.
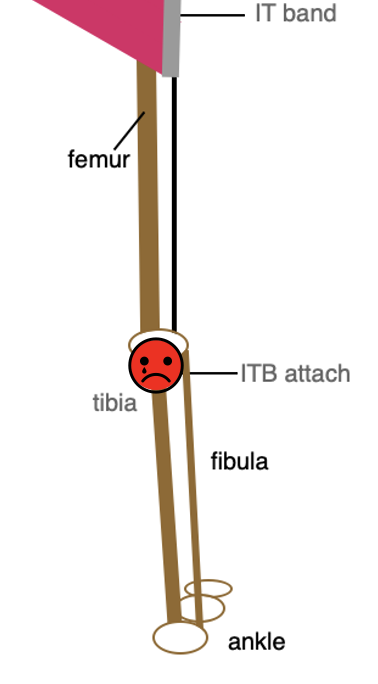
ITB Syndrome Pain
Muscle Geek Alert
The iliotibial or IT band originates from two muscles in the hip (ilium). Is it a tendon or a ligament? It’s both. A tendon attaches muscle to bone with straight fibers continuing from the muscle direction. Ligaments, which attach bone to bone, are made up of criss-cross collagen fascia, built for strength and used to stabilize a joint. ITB tissue looks and acts like a ligament, but attaches two hip muscles to the tibia. So for a hybrid tendon/ligament, a multi faceted approach is helpful in addressing ITB Syndrome. What are the various anatomical elements in ITB Syndrome?
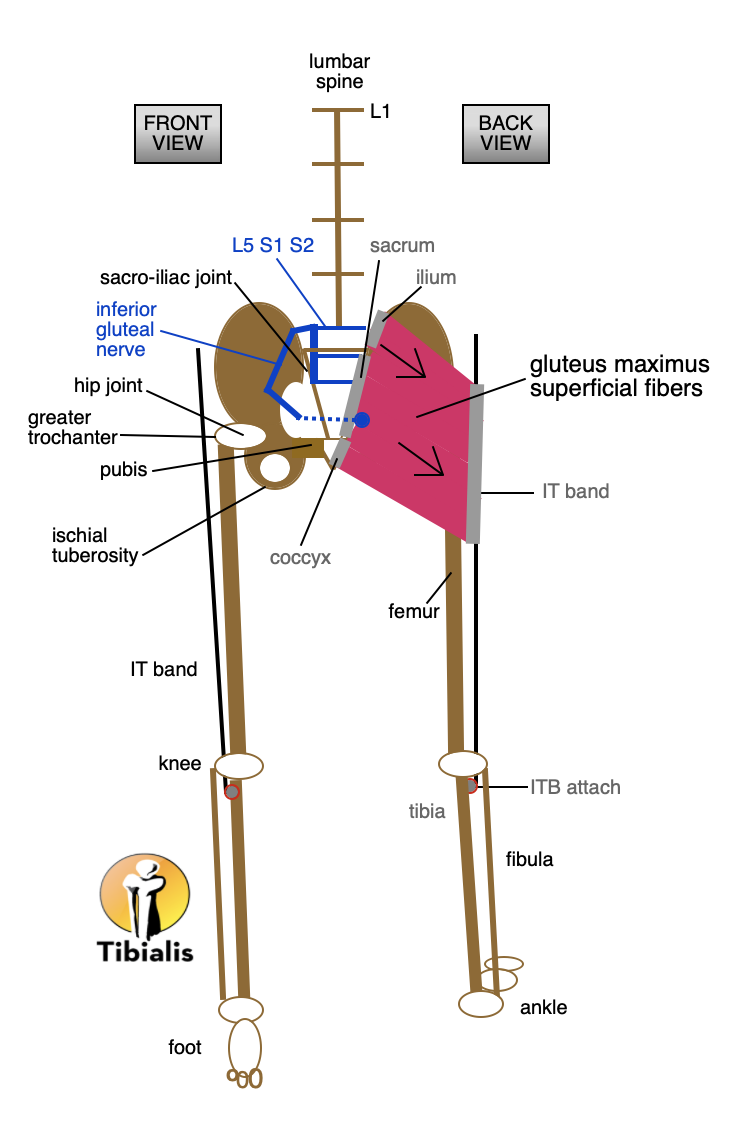
Gluteus Maximus Superficial Fibers
Direct Attachments – Muscles of the IT Band
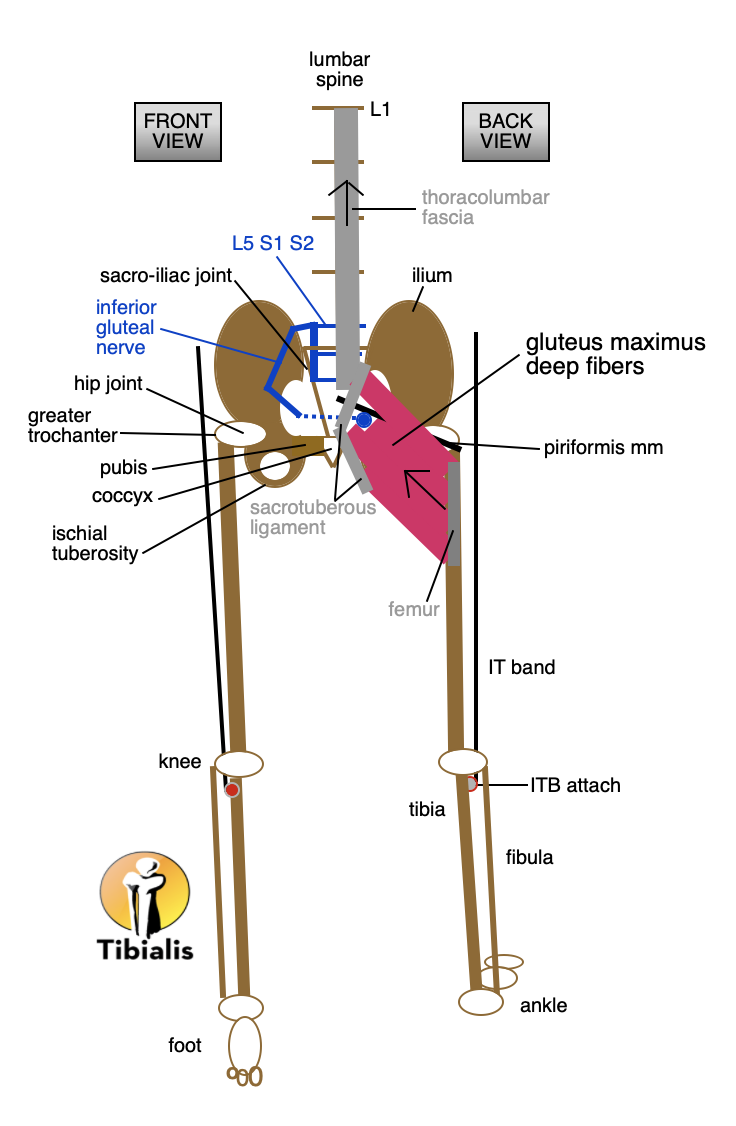
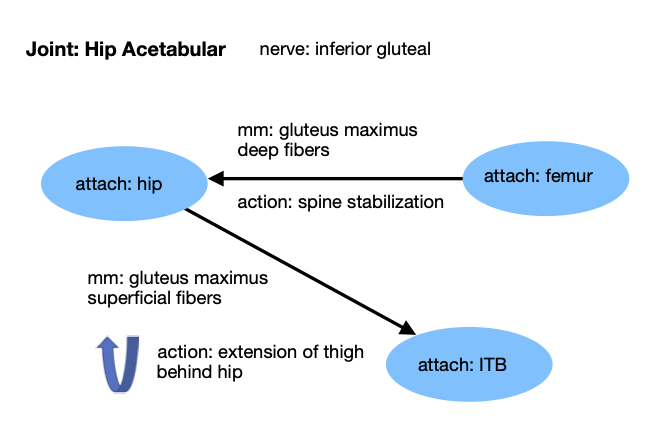
Gluteus Maximus The ilium, sacrum and coccyx or tailbone have superficial fibers of the gluteus maximus that attach directly to the IT band. The primary action of these fibers is hip extension which brings the thigh behind the body when walking or running. The gluteus maximus is innervated by the inferior gluteal division of the sciatic nerve.
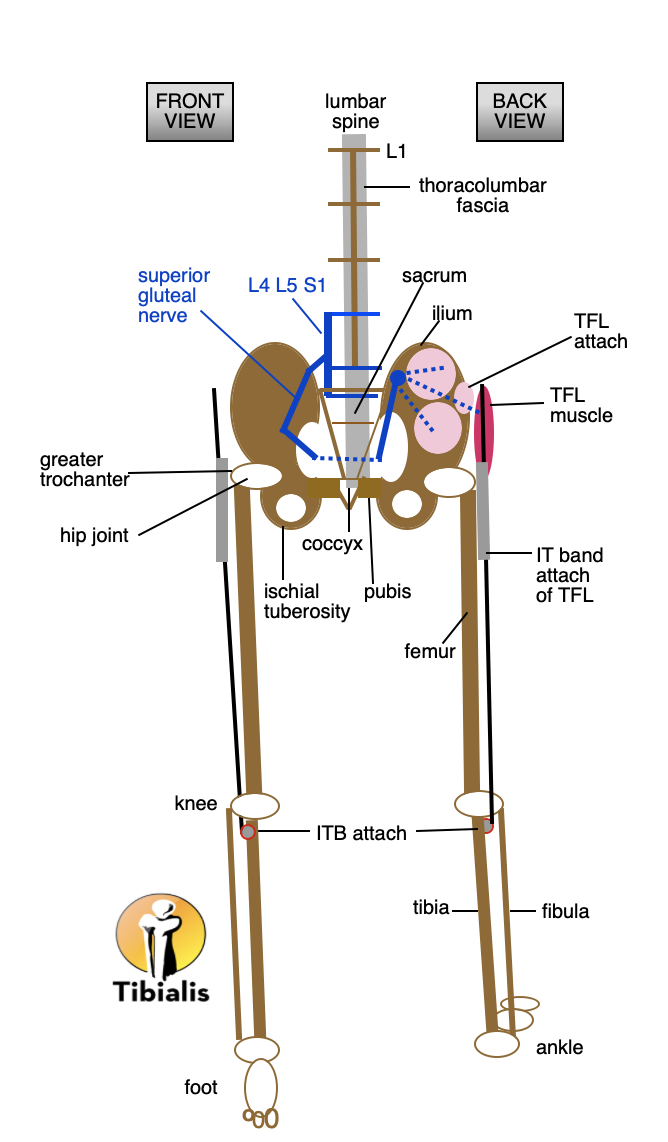
ITB attach of TFL
Tensor Fasciae Latae or TFL The TFL attaches to the iliac crest of the ilium and converges with the gluteus maximus into the ITB below the greater trochanter.
Other Muscles Related to Direct Muscles of IT Band via Common Nerve
The TFL is innervated by the superior gluteal nerve, which also innervates the gluteus medius and gluteus minimus. All three of these muscles work together as a special team for hip joint abduction of the thigh. The TFL has a direct connection to the ITB, but the other gluteal muscles are indirect contributors or potential sources of ITB pain or restriction.
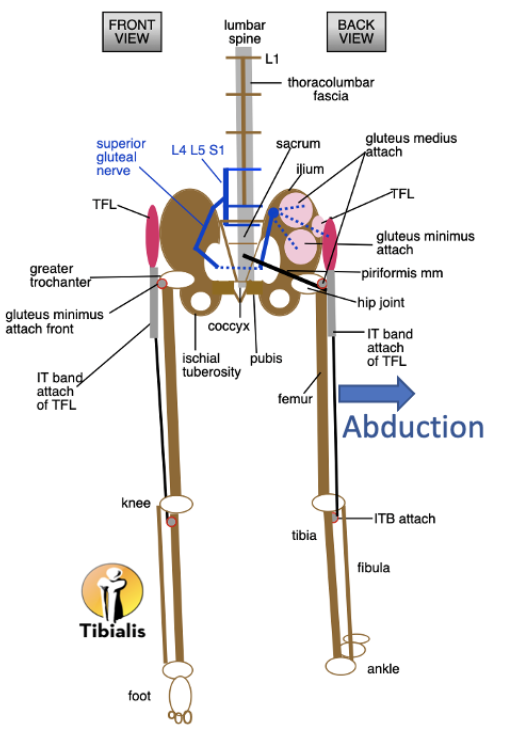
Superior Gluteal Nerve Abduction Muscles
Muscles with Similar Functions to ITB
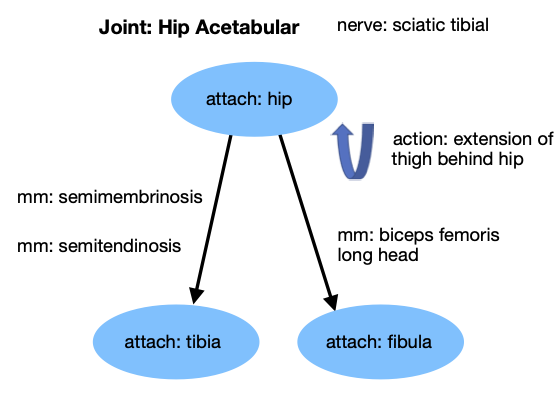
Hamstrings
Both the hamstrings and the gluteus maximus superficial fibers work to extend the thigh behind the hip. Hamstring muscles are strong and can substantially influence the stability of the hip joint. If the joint stability is disrupted, the IT band will need to work harder to maintain steadiness.
Gluteus Maximus Deep Fibers
Gluteus Maximus
The deep fibers of the gluteus maximus act on spine stabilization which, when compromised, can also discombobulate movement patterns that can strain the IT Band.
Hamstring Attachments
Proximity to Attachment Site of Tibial Attachment of IT Band
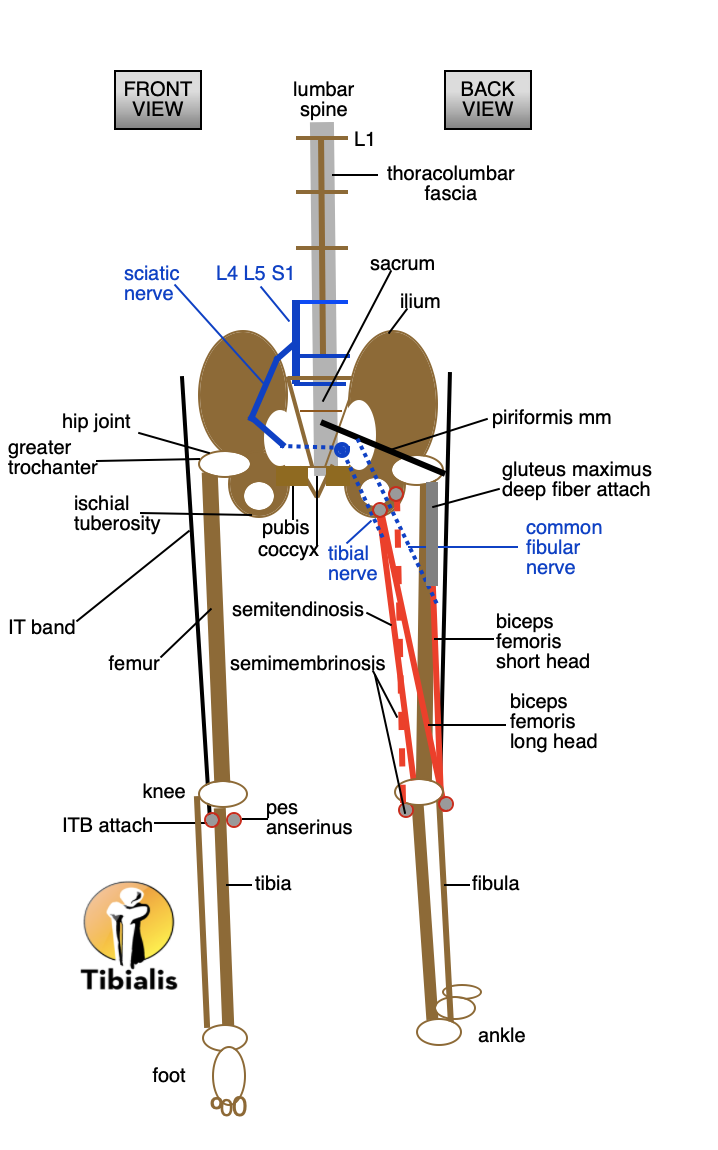
The short head attachment of the biceps femoris to the posterior linea aspera of the femur is in a direct line of attachment to the deep fibers of the gluteus maximus acting on hip and spine stabilization.
The line of the fibular nerve stabilizes motion from the foot to the hip in conjunction with the ITB.
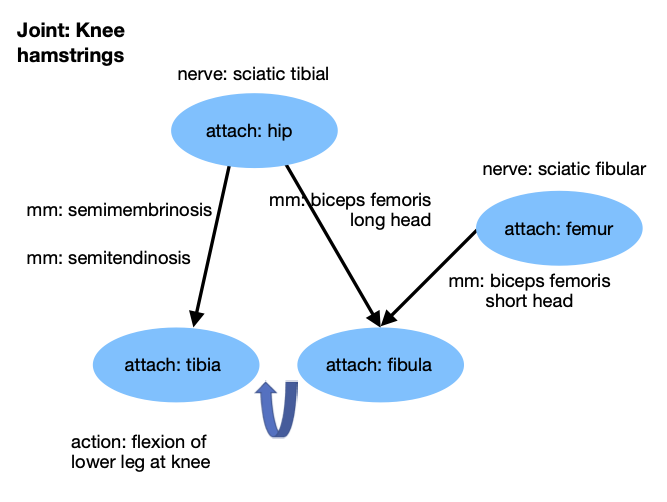
Hamstring Attachments at Knee
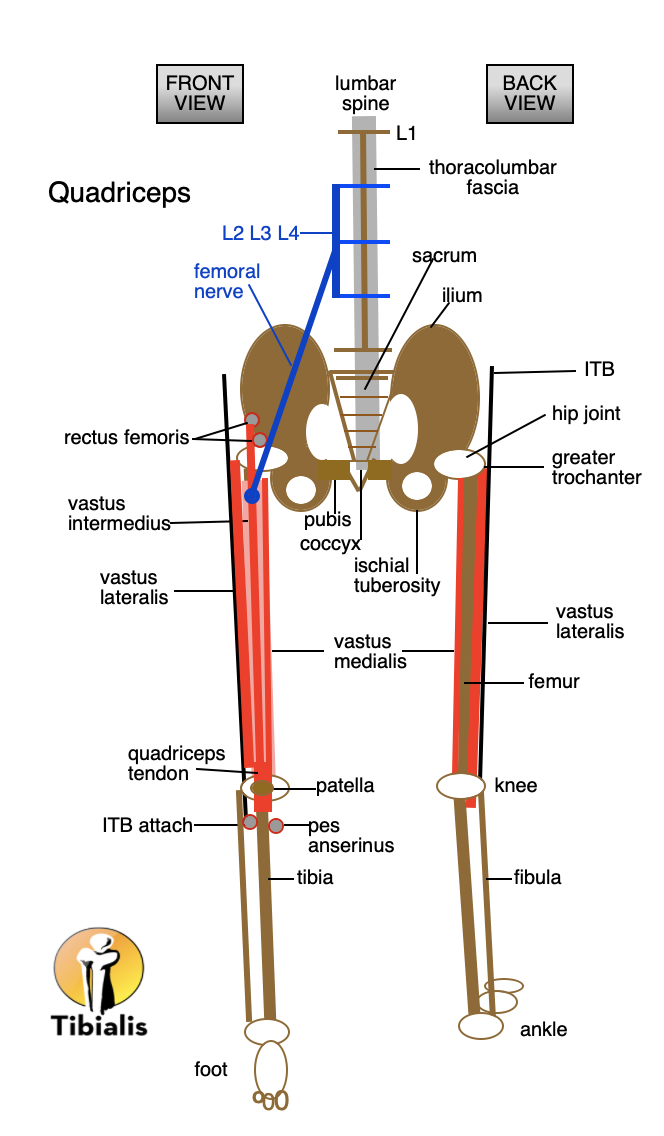
Quadricep Attachments
The vastus lateralis muscle of the quadriceps is attached along the entire linea aspera of the posterior femur directly lateral to the connected vertical line
of the gluteus maximus deep fibers and short head of the biceps femoris. The vastus lateralis muscleis directly under the IT band.
The ITB attaches to the lateral condyle of the tibia.
Other muscles that attach in that general area are:
- Combined biceps femoris attachment at the head of the fibula
- Lateral gastrocnemius which crosses the outer knee from the lower leg
- Popliteus which crosses the back of the knee from the lower lateral femur to the upper medial tibia
- Soleus attaches to fibula and tibia, extends to achilles tendon to heel
- Tibialis anterior from lateral condyle of tibia to medial cuneiform and big toe metatarsal
- Fibularis longus from top of fibula to medial cuneiform in foot
- Extensor digitorum longus from the lateral condyle of tibia to femur to top of toes in foot
Level 5: Cross Body Function
The ITB is primarily a stabilizer of the hip and knee. If there are issues on the other side of the body or somewhere in the torso, it may require the IT Band to work harder. The constant pulling of the ITB from multiple areas creates a gap between the tendon of the muscles and the attachment site on the bone. Calcium is sent as a patching material to the overworked area at the tibia to fill in the gap which creates irritation and pain.
Opposing muscle group restricted function may limit efficient movement patterns. The hamstrings in the back of the leg do knee flexion. The quadriceps in front of the leg do knee extension. If one or both of the muscle groups is weak or overworked, the communication of motion through the knee can be compromised. Fascia is intertwined throughout the body. The directional forces of the motor neurons of muscular movement will set in motion sensory neuron responses from multiple sources which are read by fascia to establish resting muscle length, posture and balance relative to the new position after movement. This could explain why activity anywhere in the body can improve overall health of the entire physique. A graceful ballet dancer or a spinning shot putter has connected all of the muscle, nerve and fascia dots to gain complex access to whole body power. A failure anywhere in the body can make the difference between ending your run in semi-finals versus finals.
ITB Issues that May Require Medical Attention
The IT Band roughly correlates to the gall bladder meridian indicating a systemic issue.
Fracture of the tibia or fibula can be painful in the ITB attach area.
A meniscus or ligament strain at the knee can be involved.
A baker’s cyst behind the knee is uncomfortable.
Bursitis at the greater trochanter of the femur can irritate the ITB from the upper muscles crossing the bursa. IT Band Syndrome eventually limits activity due to the intensity of the pain.
A comprehensive treatment plan addressing the various levels of potential anatomical element involvement can get you back to your adventurous self.
Aut![]() hor: Mary Bai of Tibialis, LLC is a Certified Massage Therapist practicing Medical Massage in Redwood City, CA.
hor: Mary Bai of Tibialis, LLC is a Certified Massage Therapist practicing Medical Massage in Redwood City, CA.
Contact: mary@tibialis.com